Abstract
Expenditures on health care and education sector constitutes large proportion of government expenditures in almost all countries. So the question arises: Do we really need to spend that much or not? This paper tries to find the effectiveness of public expenditure on two sectors mentioned above. As effectiveness indicator in health – life expectancy and mortality rate are used and in education school enrollment. This paper focuses on Azerbaijan government expenditure covering the years 1995-2011. Findings suggest that public expenditure does not play significant role in increasing effectiveness of both sectors. But it still does not mean that we do not need public expenditure on these sectors at all.
Key words: public expenditure, health care, education, effectiveness
Introduction
One of the main functions of any government is to provide its population with public goods and services. A public good is a product that one individual can consume without reducing its availability to another individual and from which no one is excluded. Education and health care can be treated as public goods, although in many countries private sector comes in, still in order to avoid under-provision problem, the biggest proportion of these goods are provided by the government. Azerbaijan is one of such countries.According to 2012 indicator Azerbaijan’s public expenditure on education constituted 2.8% of overall GDP which is average in comparison with all world countries (Human Development reports, 2012). Although education is not pure public good, there are reasons for government involvement as it causes potential productivity spill overs, more informed and less criminally inclined citizens. Higher level of education lead to lower rate of behaviours such as smoking, drinking which at the end also leads to healthy labour force, healthy voters both in terms of physical and mental means, overall healthy population. Also in global level, a number of millennium development goals are directly related to education and health such as: achieve universal primary education,reduce child mortality,improve maternal health andcombat HIV/AIDS, malaria and other diseases(The role of public expenditure in the provision of education and health, 2003).
The other reason why health care and education is mostly provided by the government is ensuring equity. The government does not want the poor to be hindered from using such services for the lack of income. Because having education has always been compelling interest of each state. Therefore these two services that are provided by government are either free or are at more affordable price in comparison with private sector.
Countries can gain numerous benefits from having a highly educated and healthy population. Social programmes such as health care and education are generally believed to have a bearing on human development and consequently increased government spending in those programmes is expected to result in better social outcomes. Over many years, researchers have argued that higher human capital is associated, among other things, with higher economic growth (Suryadarma, 2012). Therefore government spends so much on education and health care system as it is expected to play significant role in overall development.
How to evaluate performance on education and health care system: through effectiveness or efficiency? Being effective means accomplishing a purpose; producing the intended or expected result whereas being efficient means performing or functioning in the best possible manner with the least waste of time and effort(Goh, 2013). There are 2 dimensions of efficiency: technical and allocative(Ulrike Mandl, 2008). Technical efficiency measures the pure relation between inputs and outputs taking the production possibility frontier into account. Allocative efficiency reflects the link between optimal combination of inputs taking into account costs and benefits and output achieved. In order to analyze effectiveness and efficiency we need to determine inputs, outputs of the process correctly. Also we should be able to distinguish output and outcome. Outcome carries broader meaning than output. For example, secondary education quality is output where to form competitive labor force is outcome. Different outputs can serve to one specific outcome. Identification of inputs and outputs in public sector is difficult. Because they are interlinked, one sector’s output can be the other one’s input. Public spending efficiency can be affected by different factors, such as institutional, structural, country-specific features, even environmental factors. Different countries use different methods. For example, United Kingdom employs the ratio of real output to real input. As mentioned above, efficiency is not directly measured. Because almost all of the public sector products are not sold, this means that price data are not achievable.The main assessment tool of efficiency is input-output ratio, which means that the greater output for a given input you have, the more efficient you are. Referring to Ulrike Mandl, efficiency indicates feasible output levels given the scale of operations. Effectiveness shows the success of the resources used in achieving the objectives set. As efficiency is hard to measure and effectiveness is more relevant to my research purpose,I will try to analyze effectiveness of public expenditure on health and education.
Literature review
Public spending affects the performance of public sector. Because high public spending limits the maneuver ability of the government, also reveals the priority of economy and the focus of the state which means that whether the state wants stabilization, growth or adjustment. There are several factors which influence public spending effectiveness: administration, education, health, income distribution, economic stability and economic performance outcomes. The investigation by Afonso, which is over EU countries shows that, as the size of public sector is small, public services are more effective. Referring to Afonso the security of property rights, educational level affect public spending effectiveness positively. Former researches show that, there is no clear connection between spending on education and the observable performance of pupils. There are other factors that can influence effectiveness of spending on education, which are school size, the ratio of teachers to pupils, residency-based selection of pupils, even education of parents. Public spending on both education and R&D aims to be more productive and to grow.
Education and health service is not only desirable to individuals, but to society as a whole. Because educated people create positive externality, if one professor intends something good, not only he himself, overall population, maybe even global society can benefit from it, for example, discovering cure of any disease. Therefore any government spends much on these aforementioned sectors and it is expected to increase effectiveness. But there are differences between theoretical and empirical results. According to theory there is positive relationship between public expenditure on education and health with effectiveness. However empirical results in this field are mixed. There is not unanimous finding. In order to measure the effectiveness of public spending on health, Emanuele Baldacci uses child mortality as dependent, government expenditure on health as independent variable on his study(Baldacci, 2003). For education sector he uses primary and secondary school enrollment as the indicator of effectiveness and public spending on education as influencing factor. His paper claims that public spending on education does not alone affect effectiveness;he evaluates other variables’ influence as well. This study finds out that per capita income and public expenditure on education has positive correlation. Adult illiteracy has negative, urbanization has positive, and fertility rate has negative effect on population’s literacy level. Also according to his paper as share of girls enrolled in secondary education increases effectiveness of government expenditure increases simultaneously. He claims that income is a more important determinant of the population’s health status rather than public spending(Baldacci, 2003).
Roland Craigwell in his study employs life expectancy at birth as dependent variable and public spending on health as independent variable and finds positive correlation between them(Craigwell, 2012). Among other independent variables he refers to DPT (diphtheria, pertussis and tetanus) immunization, access to improved sanitation facilities and water and reveals positive relationship between them and effectiveness. On education side of his analysis he uses primary and secondary gross school enrolment in percentage as the effectiveness indicator, government expenditure on education as independent and influencing variable. One of his important findings is that effectiveness on health and education is intertwined because improvement in infant mortality increases school enrolment which shows effectiveness in education sector(Craigwell, 2012).
Daniel Suryadarma uses two sets of data as effectiveness in education sector which areschool enrolment and national exam results. The results show that public spending on education increases enrollment rate, however does not affect national exam results. Therefore he claims that this result does not mean that there is no need for public spending, but instead it should be accompanied by other policies, such as improving curriculum, recruiting higher-quality teachers(Suryadarma, 2012). In other study by Svetlana Batare, Latvia with EU countries are compared and the author argues that, as educated people are public good, private sector is unwilling to produce more of them and support education sector. Therefore in education sector, public spending’s role is irreplaceable(Batare, 2012).
Andrew Raj Kumar’s study covers 91 developed and developing countries. As Baldacci, his findings also prove that there is no direct, significant relationship between public spending on education and education achievements or public spending on health and improvements of health care system(Rajkumar, 2008). The main determinant is income. The impact of government expenditure in poorer countries is stronger than wealthier ones. He explains the reasons why public spending is not so efficient in terms of institutional quality, governance indicators and claims that they are much more important. The author interact public health spending variable with governance indicator (corruption) or quality of bureaucracy. He uses child mortality as effectiveness indicator in health sector and education attainment in education sector which is defined as the number of proportions of school-age children that enter and complete primary or secondary school. He got 2 results from this model: Students in rich countries have higher education attainment. The link between public education spending and education attainment is strengthened with improved governance(Rajkumar, 2008).
Methodology
After doing literature review I will try to find the relationship between effectiveness indicators in health care and education sphere and public expenditure in these fields respectively. In this paper I will use the data related to Azerbaijan from the World Bank(The World Bank). This data cover the years 1995-2011 (as some data were missing in years 2012-2015, these years are not included). As effectiveness indicator in health care sector I refer to life expectancy and mortality rates (both under the age of 5 and infant mortality) expecting as public expenditure in health sector increases, life expectancy will increase whereas mortality rate under age 5 will decrease. Based on literature, school enrolment rate will be used as effectiveness indicator in education sector and will try to find its relationship with public expenditure on education.Also as income level indicator GDP per capita is included to the analysis and will try to find its relationship with effectiveness in both sectors. I will use STATA statistical analysis program for my calculations. I will apply 95% confidence level in my analysis.
Results
Health care sector
Health outcomes are a function of a wide variety of factors – economic, social, cultural, geographical and environmental, as well as on health sector interventions. Econometric evidence shows that most cross-country variance in outcomes is explained by per capita income (poverty level) differences and that public expenditure has limited explanatory power. So we will see how it is applicable in Azerbaijan.
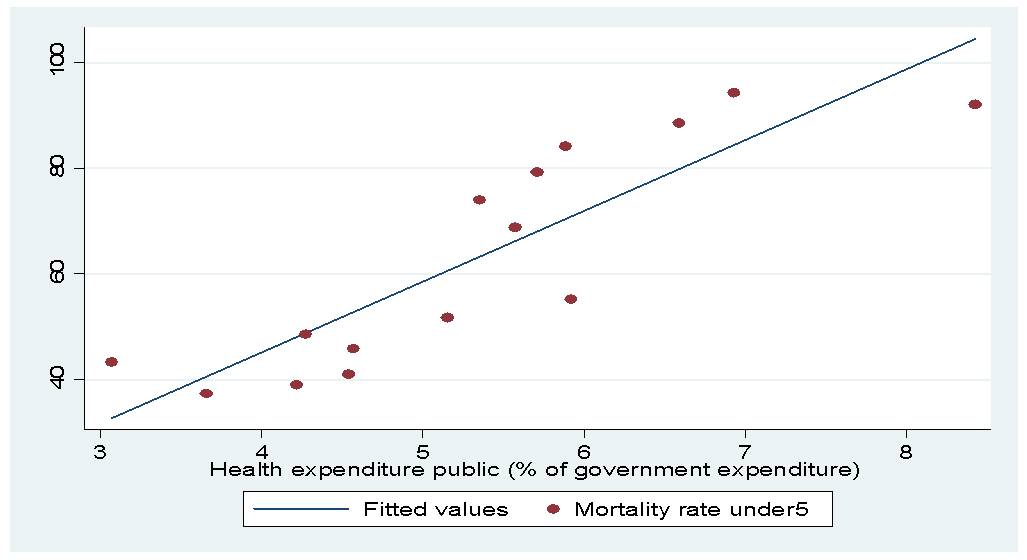
I got so interesting results in health care sector. I found that there is negative correlation between life expectancy and public expenditure on health (table and graph 1) which was quite significant. As unexpectedly, positive relationship was observed between mortality rate and public expenditure on health (table and graph 2). It means that as public expenditure on health increases, life expectancy decreases and vice versa as public expenditure on health care increases mortality rate also increase (it is applicable for both mortality rate under the age of 5 and infant). These results show that there is no direct positive relationship between public expenditure on health and effectiveness in this sector.
Table 1

Graph 1
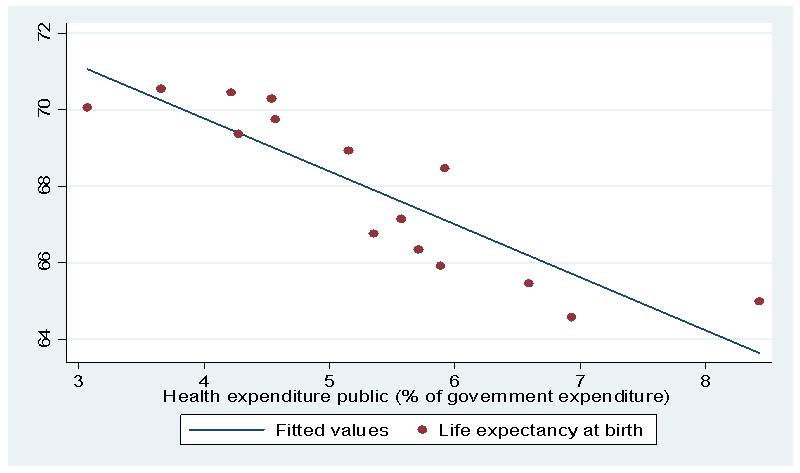
Table 2

Graph 2
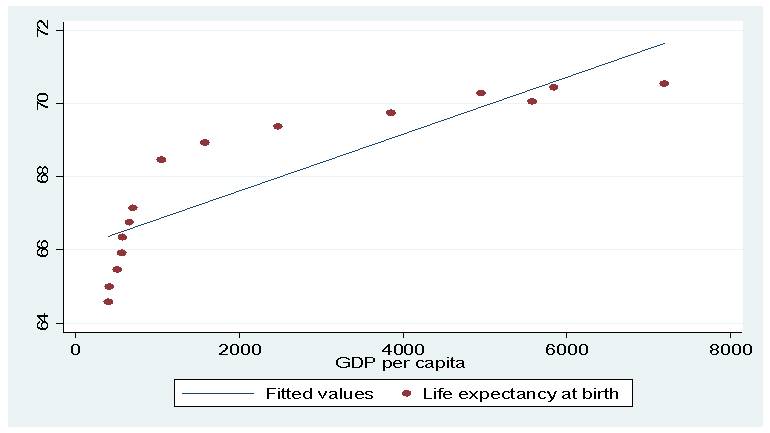
As mentioned in literature review, some scholars claim that not exactly public expenditure matters on effectiveness, however income level matters. Therefore I included GDP per capita as income level indicator and found that there is positive relationship between income level and being healthy (Graph 3). As GDP per capita increases by one unit, life expectancy is increasing 0.001 units. Because health care is normal good, which means that as income increases, consumption of this good is growing which leads to receiving more and high quality service and results in increasing effectiveness of health.
Graph 3
Different from health sector, in education positive relationship is observed between effectiveness and public expenditure on education where effectiveness is indicated as school enrolment rate (Table 3). But it still is not strong proof, because p>α (0.477>0.05) which means that our result is not significant. Therefore we cannot confidently claim that as public expenditure on education increases by one unit, school enrolment increases by 1.701 units.
Table 3

As done in health care sector, in education also GDP per capita is used as influential variable to effectiveness in education (here school enrolment rate). Because we know that education is also normal good (consumption is increasing as income rising). But here negative correlation was observed between GDP per capita and school enrolment rate which is also insignificant result, because 0.963>0.05 (table 4). Therefore we cannot claim that GDP per capita does not affect effectiveness in education positively, which means that just our data is not representative.
Table 4

Summary of results and recommendations
Our results show that public expenditure on health and education does not increase effectiveness that much. But it does not mean that we do not need public expenditure at all. This ineffectiveness can be explained by the focus on increasing quantity rather than quality. For example, according to the interview with the official of local administration in Ordubad city, new hospitals are built there and provided with modern medical equipment, but there are no specialized and trained doctors to use them (Ceyhun Abdulla, personal communication, 15.11.15). Therefore, when guest doctor comes from Baku to Ordubad, there is always a long queue in front of this doctor’s room.It shows that even there is difference between quality level among cities and rural areas. Also we see that public expenditure is spent on quantity issues as buying equipment, repairing etc.
Regardless these results public spending should exist. According to organizational behaviour theory, an organization can be publicly owned and funded, publicly owned while privately funded, privately owned but publicly funded and privately owned with private funding(Hal, 2014). In order to increase effectiveness and efficiency, we need more publicly owned and privately funded health and education companies. Therefore proper environment should be created for private sector’s entrance. For example, ADA University of Azerbaijan is publicly owned education centre, however funding is provided by different local and international private organizations such as Azercell, SOCAR, British Council, Bank of Baku etc and the quality level of service is quite high in comparison with other public universities(ADA Foundation, 2011).
Other recommendation in order to increase quality of education and health care system can beattracting talented, skilful teachers and doctors to remote regions via different incentives as higher salary, release such teachers and doctors from paying communal fees, providing them with land, free check-up once a year etc. would be useful to solve the lack of talented and educated personnel problem in the regions.
Conclusion
According to our calculations we can claim that public expenditure on health care and education does not matter to great extent. Because public expenditure just adresses to increase quantity of service, for example due to public expenditure on health care new hospitals are built, new medical apparatus are bought. But if nobody can use these equipment then what is the point in spending that much? Also corruption plays important role in ineffectiveness. Government intends to send exact amount to education or health care but which proportion actually reaches needy point is questionable. Therefore this paper claims that public expenditure should not be spent for increasing quantity, but quality. For example, public expenditure on education and health care should be accompanied by training of teachers and doctors, increasing quality of institutionalization. Alsothe quality of institutions should be increased which entails decreasing corruption. Thus, in governmental level such calculations should be done and the optimal level of public expenditure should be determined. Also in order to increase efficiency the government should let the private sector enter. At the same time the government should have proper regulatory regimes in place to maintain education and health service standards. Thus, by improving governance, resources can be saved and utilized to improve access to and the quality of education and health services. More effective implementation of checks and balances and greater decentralization in the provision of education and health services can help to check the wastage and the leakage of resources(The role of public expenditure in the provision of education and health, 2003). The officials should remember that: Quality matters, quantity not!
By: Leyla Abbasli
References
The role of public expenditure in the provision of education and health. (2003). Economic and Social Survey of Asia and the Pacific 2003. United Nations.
ADA Foundation. (2011). Retrieved November 26, 2015, from http://www.adafund.org/site/donors
Human Development reports. (2012). Retrieved November 23, 2015, from United Nations Development Programme: http://hdr.undp.org/en/content/expenditure-education-public-gdp
Baldacci, E. (2003). More on the effectiveness of public spending on health care and education. Journal of International Development, 709-725.
Batare, S. (2012). Efficiency of public spending on education. PUBLIC POLICY AND ADMINISTRATION, 171-186.
Craigwell, R. (2012). Effectiveness of government expenditure on education and health care in Carribean countries. International Journal of Development Issues, 4-18.
Goh, G. (2013, August 9). Insight Ssquared. Retrieved November 15, 2015, from http://www.insightsquared.com/2013/08/effectiveness-vs-efficiency-whats-the-difference/
Hal, R. (2014). What Make Public Organizations Distinctive. In R. Hal, Understanding and Managing Public Organizations (p. 72). Somerset,NJ: John Wiley & Sons.
Rajkumar, A. (2008). Public spending and outcomes: Does governance matter? Journal of Development Economics, 96-111.
Suryadarma, D. (2012). How corruption diminishes the effectiveness of public spending on education in Indonesia. Bulletin of Indonesian Economic Studies, 85-100.
The World Bank. (n.d.). Retrieved November 23, 2015, from http://data.worldbank.org/
Ulrike Mandl, A. D. (2008). The effectiveness and efficiency of public spending. European Economy.
